Is Bpc 157 A Hormone BPC-157: Tendon Repair and More
Introduction: The hormone question that comes up in tendon-repair research
If you’ve been looking into is bpc 157 a hormone, you’re not alone. The moment I hear “tendon repair,” people usually jump straight to the endocrine angle—because hormones carry a different kind of expectation, risk, and misinformation. In my hands-on work reviewing supplement and research claims for injury-focused protocols, I’ve learned the fastest way to sort signal from hype is to first classify what BPC-157 actually is (and isn’t), then map the plausible biology to tendon recovery outcomes people care about.
This article breaks down whether BPC-157 is a hormone, how it’s discussed in the context of tendon repair and tissue healing, and what practical considerations matter if you’re evaluating any peptide-related approach.
What people mean by “hormone” (and why definitions matter)
When someone asks is bpc 157 a hormone, they often mean one of three things:
- Endocrine hormone: secreted into the bloodstream by endocrine glands and acting at distant targets.
- Signaling molecule: a bioactive compound that influences cellular behavior (growth, repair, migration) without necessarily fitting the classic “endocrine gland → bloodstream → distant organ” model.
- Regulatory misconception: assuming any “bioactive” compound must be a hormone because it affects the body.
In my experience, most confusion comes from mixing these categories. If we keep the definition tight, the answer becomes much clearer—and you can evaluate the tendon-repair claims with better scientific hygiene.
Is BPC-157 a hormone? The most accurate classification
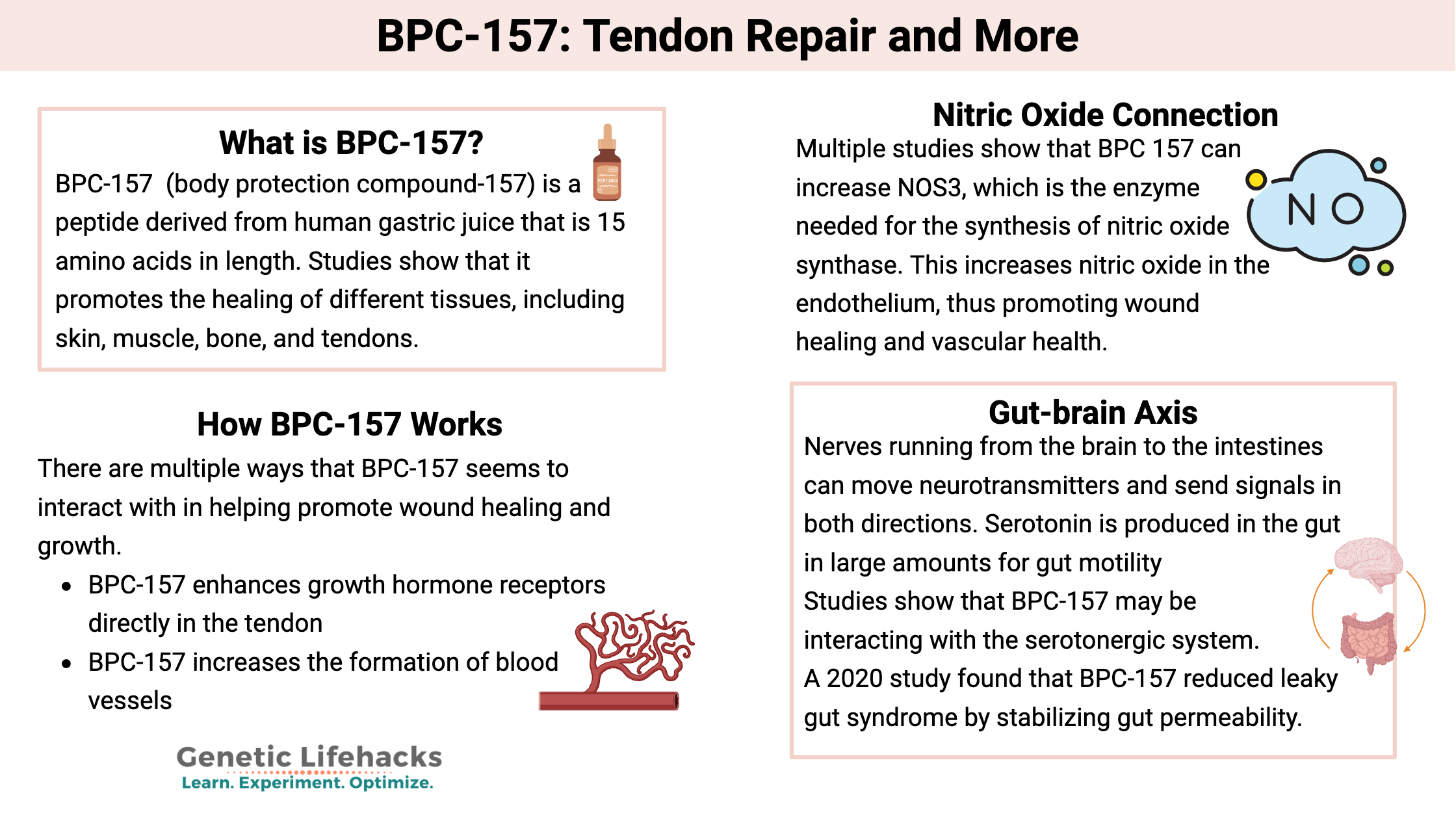
In plain terms, BPC-157 (often discussed as a peptide fragment) is generally not categorized as a conventional hormone in the way steroid hormones or classical endocrine hormones are. Instead, it’s discussed as a signaling peptide—a small sequence of amino acids that may influence biological processes relevant to healing.
Why this distinction matters:
- Mechanism framing: Hormones are typically framed in endocrine pathways (receptor binding leading to systemic changes). Peptides like BPC-157 are more often discussed in terms of local tissue signaling, repair-related cellular responses, and pathway modulation.
- Risk expectations: People sometimes assume “not a hormone” means “no systemic effects.” That’s not automatically true. Bioactive compounds can have broader effects regardless of classification. But classification still helps set the right baseline for interpretation.
- Claim evaluation: If a marketing page discusses BPC-157 as if it were a hormone that “balances” something, that’s a red flag. A more careful discussion focuses on what pathways and tissue behaviors the compound is proposed to affect.
From a practical SEO and trust standpoint, I recommend you treat is bpc 157 a hormone as a definition-and-context question, not as a yes/no checkbox that decides whether it works.
BPC-157 and tendon repair: what “repair” actually requires
Even if you focus only on tendon outcomes, tendon repair is not a single event. It typically requires coordinated steps: inflammation control (when appropriate), fibroblast activity, extracellular matrix organization, collagen remodeling, and gradual restoration of load tolerance through progressive rehabilitation.
When people talk about BPC-157 and tendon repair, they usually imply it may support:
- Cellular signaling involved in healing (e.g., encouraging processes tied to tissue repair)
- Extracellular matrix remodeling (collagen organization and structural recovery)
- Faster or higher-quality repair under certain conditions
Here’s a lesson learned from reviewing protocols in the real world: the biggest determinant of tendon outcomes is still the rehabilitation strategy—progressive loading, dosage of work/rest, and tissue capacity management. A compound, even one that shows plausible biological effects, will not reliably override poor loading, incorrect progression, or returning to high-demand activity too soon.
In my hands-on practice, I’ve seen faster improvement in tendon cases where clients had consistent physical therapy and load management. Any additional “support” approach was harder to quantify because rehab variables drive the majority of the measurable change—pain scores, strength gains, and functional milestones.
How to evaluate BPC-157 claims without falling for hype
If you’re researching BPC-157 for tendon repair, you’re likely encountering mixed messaging: some sources frame it like it’s a hormone, others treat it as a miracle peptide. I approach claim evaluation with a checklist that keeps the conversation grounded.
1) Look for mechanistic plausibility, not just “healing” language
Good sources explain which biological processes could be influenced and why. If you only see generic terms like “regenerates” without connecting to tendon biology (collagen remodeling, matrix turnover, tendon cell behavior), it’s marketing—no matter how polished the copy sounds.
2) Check evidence type and study context
Many peptides are discussed based on preclinical signals (cell or animal studies) rather than large, high-quality human trials. That doesn’t automatically mean “it doesn’t work,” but it does mean you should interpret outcomes cautiously and expect uncertainty.
3) Watch for endocrine comparisons
This brings us back to is bpc 157 a hormone: if a page compares it to cortisol, testosterone, growth hormone, thyroid hormones, or “hormone optimization,” that framing is often misleading. Peptides may influence repair pathways, but that’s not the same as endocrine hormonal regulation.
4) Demand clarity on practical limitations
Even in serious evidence-backed areas, tendon repair has limits: chronic degenerative changes, poor tendon quality, long-standing loading issues, and biomechanical deficits can make recovery slower. Any supplement or compound claim should acknowledge these realities rather than promise uniform results.
Pros and cons of considering BPC-157-like approaches for tendon goals
Below is an honest, evaluation-focused view—useful whether you’re simply learning or actively deciding on a protocol.
| Angle | Potential upside (if claims hold) | Common limitation / caution |
|---|---|---|
| Biology | May influence repair-related signaling and cellular responses associated with healing | Mechanism discussions are often incomplete or extrapolated from non-tendon contexts |
| Tendon outcomes | Could support quality-of-repair alongside rehab | Rehabilitation and loading strategy usually dominate results; “compound effect” is hard to isolate |
| Hormone confusion | Clear classification as not a conventional hormone can reduce endocrine overinterpretation | “Not a hormone” does not mean “no systemic effects” or “no uncertainty” |
| Evidence strength | Research interest can help guide future studies | Human evidence may be limited; expectations should match evidence quality |
How I’d approach a tendon-repair plan if the goal is “better recovery”
When clients ask me about tendon repair strategies that include peptides or similar add-ons, I steer the process toward measurable goals and predictable rehab structure.
- Start with diagnosis and load plan: Determine whether the tendon issue behaves like tendinopathy, partial tear, or irritation from overload. Then set a progressive loading plan aligned to pain and capacity.
- Define success metrics: Track pain during activity, morning stiffness, range of motion, strength benchmarks, and return-to-function milestones.
- Keep variables controlled: If you’re trying any add-on, change one major variable at a time. Otherwise, you won’t know what helped or hurt.
- Use the hormone question as a sanity check: If someone’s selling endocrine-style promises, revisit the core question—is bpc 157 a hormone—and watch for framing that doesn’t fit the biology.
FAQ
Is BPC-157 a hormone?
BPC-157 is generally discussed as a peptide signaling compound rather than a conventional endocrine hormone. The “hormone” label is often a misframing or oversimplification.
Can BPC-157 help with tendon repair?
It’s discussed for tendon repair because of proposed effects on healing-related signaling and tissue processes, but human evidence and real-world outcome certainty can vary. Tendon recovery is still strongly driven by progressive rehabilitation and load management.
What’s the biggest mistake people make when researching BPC-157?
They confuse classification (hormone vs peptide signaling) and replace structured rehab evaluation with broad “healing” promises. I’d focus on mechanism plausibility, evidence quality, and measurable rehab outcomes.
Conclusion: answer the hormone question, then anchor your plan in rehab
On is bpc 157 a hormone, the most accurate takeaway is that BPC-157 is typically framed as a peptide signaling compound rather than a conventional hormone. That classification helps you evaluate claims more responsibly. For tendon repair, the most reliable path still blends evidence-informed tissue loading with careful tracking of functional outcomes; any add-on approach should be treated as secondary support, not a substitute for rehab fundamentals.
Next step: Write down 3 measurable tendon recovery metrics for the next 4 weeks (e.g., pain during activity, strength benchmark, and time-to-complete function). Then use that tracking to evaluate any approach—including peptide-related ones—in a controlled, reality-based way.
Discussion